Get the free empty denal claim form
Show details
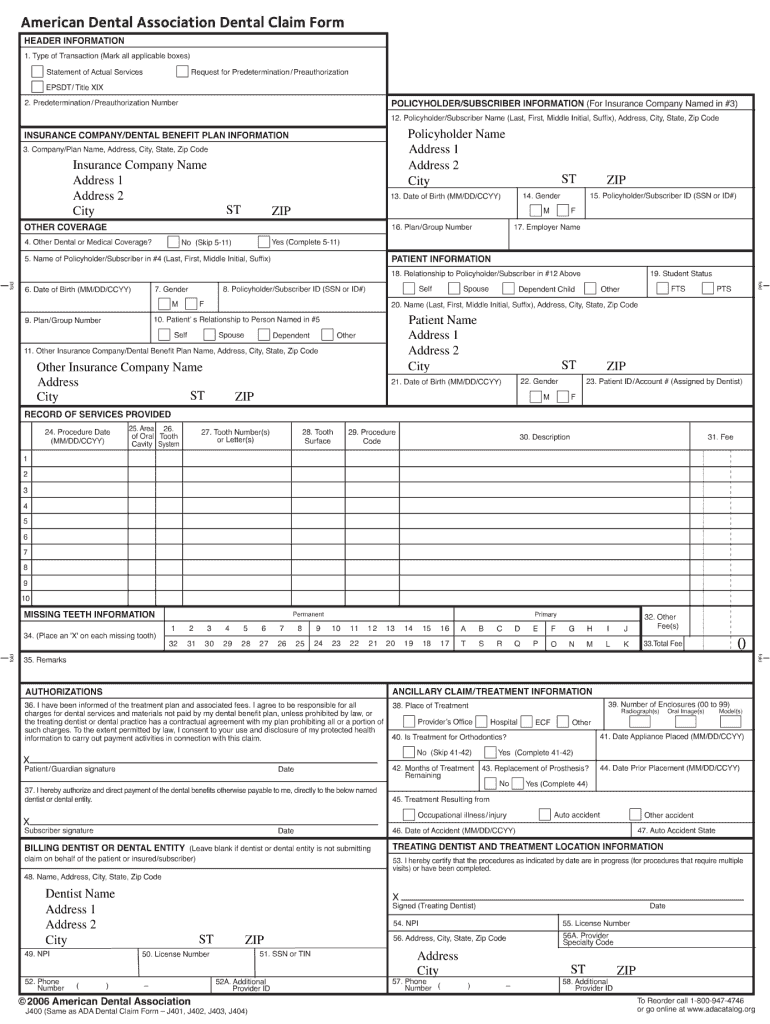
HEADER INFORMATION Dental Claim Form Request for Predetermination / Preauthorization 1. Type of Transaction (Mark all applicable boxes) Statement of Actual Services EPS DT/ Title XIX 2. Predetermination
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign

Edit your empty denal claim form form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.

Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.

Share your form instantly
Email, fax, or share your empty denal claim form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing empty denal claim form online



To use our professional PDF editor, follow these steps:
1
Check your account. If you don't have a profile yet, click Start Free Trial and sign up for one.
2
Upload a file. Select Add New on your Dashboard and upload a file from your device or import it from the cloud, online, or internal mail. Then click Edit.
3
Edit blank ada dental claim form. Replace text, adding objects, rearranging pages, and more. Then select the Documents tab to combine, divide, lock or unlock the file.
4
Get your file. When you find your file in the docs list, click on its name and choose how you want to save it. To get the PDF, you can save it, send an email with it, or move it to the cloud.
With pdfFiller, it's always easy to work with documents.
How to fill out empty denal claim form

How to fill out an empty dental claim form:
01
Start by gathering all the necessary information. This includes your personal details, such as your name, address, and contact information, as well as your insurance details.
02
Next, provide the patient's information, including their name, date of birth, and insurance information if applicable.
03
Fill in the details of the dental procedure, such as the date of service, the name of the dentist or dental office, and a description of the treatment provided.
04
Include any supporting documentation, such as x-rays or invoices, that may be required by the insurance company.
05
Once all the information is filled out accurately, review the form for any errors or missing information. Make sure to double-check everything before submitting.
06
Sign and date the form, as required.
07
Finally, send the completed form and any supporting documents to the appropriate insurance company or claims office.
Who needs an empty dental claim form:
01
Individuals who have received dental treatment and wish to file a claim with their insurance company.
02
Dentists or dental offices who need to submit claims on behalf of their patients.
03
Insurance providers who require an empty dental claim form for their policyholders to submit claims for reimbursement or coverage.
Video instructions and help with filling out and completing empty denal claim form
Instructions and Help about pdfiller dental claim form
Hi my name is Gina I am an employee of a mission dental group, and today I'm going to demonstrate how to fill out a new patient packet electronically refer to the internet and type in Amos and dental group com, and you will see our web page at the top of the page select forms on this page you will see a list of various options on the left-hand side please select new patient health information this is located under electronic forms from here a new window will appear requesting your name and appointment date please fill in the requested information next you will see the new patient form screen please select the new patient pack located under new patient forms the new patient form will appear welcoming you to our practice at this point we kindly ask that you fill out our patient information form medical health history form financial policy as well as our HIPAA compliance form please take a few minutes to review the information and if you have any questions our staff members here at Amos and dental group always happy to help
Fill printable blank dental ada form : Try Risk Free
People Also Ask about empty denal claim form
How do I print a blank claim form in open dental?
How do I print a blank ADA form on Eaglesoft?
How do I print a blank ADA form?
What patient information is needed to complete a standard ADA claim form?
How do I print an itemized statement in Eaglesoft?
Our user reviews speak for themselves
Read more or give pdfFiller a try to experience the benefits for yourself
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
What is empty denal claim form?
An empty dental claim form is a blank document used by dentists to submit claims to an insurance company for payment of services provided to a patient. It usually includes information such as the patient's name, date of service, type of service, and cost. The form may also contain information about the dentist, the insurance company, and the patient's policy.
Who is required to file empty denal claim form?
Anyone who has received dental services but has not been paid by the insurance company is required to file an empty dental claim form. This form is used to initiate the claim process and provide information to the insurance provider.
What is the purpose of empty denal claim form?
The purpose of an empty dental claim form is to provide a standardized form for dentists and patients to fill out when submitting a dental insurance claim. The form includes sections for basic patient information, details of the services performed, and the amount charged for the services. It also allows the dentist to provide additional information about the services performed, such as the diagnosis or procedure codes used. By using this form, dentists can ensure that all the necessary information is included when submitting a claim, which makes the claims process much more efficient.
When is the deadline to file empty denal claim form in 2023?
The deadline to file an empty denal claim form in 2023 is typically dependent on the state in which the claim is being filed. It is best to contact the relevant state agency to determine the exact deadline.
How to fill out empty denal claim form?
Filling out an empty dental claim form can seem overwhelming at first, but it can be easily done by following these steps:
1. Gather the necessary information: You will need details such as your personal information, insurance information, and treatment details. Make sure to have your insurance card and any relevant documents handy.
2. Provide personal information: Fill in your full name, date of birth, address, phone number, and social security number on the designated sections of the form.
3. Include insurance information: Enter your insurance provider's name, address, and phone number. You may also need to provide your policy or group number.
4. Specify the treatment details: Fill in the date of service, the name of the dental provider, and their address. Indicate the procedure codes and a brief description of the services provided. If there are multiple treatments, list them separately.
5. Mention the tooth numbers: If any specific teeth were treated, note their numbers on the form. Dental charts are usually provided on the form to assist with this.
6. Include fee information: Write down the fee charged for each treatment or service rendered. This may include charges for examinations, x-rays, cleanings, fillings, or other dental procedures.
7. Indicate any relevant insurance coverage: If you have alternate insurance coverage, such as through a spouse or secondary insurance, make sure to provide those details as well.
8. Attach any supporting documents: If required by your insurance company, you may need to include supporting documents like receipts, copies of the treatment plan, or referral forms. Be sure to follow any additional instructions provided by your insurance provider.
9. Review and sign: Before submitting the form, carefully review all the information to ensure its accuracy. Sign the form and date it.
10. Submit the form: Send the completed dental claim form to your insurance company according to their preferred method (mail, fax, or online submission). Retain a copy of the form and supporting documents for your records.
Remember, it is always recommended to consult your insurance provider or ask for assistance from your dental office if you encounter any questions or difficulties while filling out the form.
What information must be reported on empty denal claim form?
When submitting an empty dental claim form, certain information must be reported to ensure accurate processing. This information typically includes:
1. Patient Information: This includes the patient's full name, address, date of birth, identification number, and contact information.
2. Dental Provider Information: It is important to provide the complete details of the dental provider or dentist, including their name, address, phone number, and any identifying numbers (such as NPI - National Provider Identifier).
3. Insurance Information: If applicable, the insurance information of the patient must be included. This includes the insurance company's name, address, and phone number, as well as the patient's insurance ID or group number.
4. Diagnosis and Treatment Details: When filling out an empty dental claim form, it is necessary to include the specific diagnosis codes (ICD-10 codes) and treatment details related to the dental procedure or service provided.
5. Dates of Service: The date(s) on which the dental treatment or service was performed must be recorded accurately.
6. Claims Attachments: Depending on the type of service, there may be requirements to include supporting documentation such as X-rays, treatment plans, or relevant medical records.
It is important to note that specific insurance companies or dental plans may have additional requirements or specific fields to be completed on their claim forms. Therefore, it is essential to review the instructions provided by the insurance company or consult with the dental provider or billing staff for the most accurate and complete information.
What is the penalty for the late filing of empty denal claim form?
The penalty for the late filing of an empty dental claim form can vary depending on the specific circumstances and the policies of the dental insurance provider. In general, insurance providers require claim forms to be submitted within a certain timeframe, typically within a few months from the date of service. If the claim form is filed beyond the allowed time limit, the insurance provider may reject the claim, and the dental treatment expenses may not be covered. Consequently, the individual may be responsible for paying the full cost of the dental services. It is advisable to consult with the specific dental insurance provider to understand their policies and any potential penalties for late filing.
How can I edit empty denal claim form from Google Drive?
By combining pdfFiller with Google Docs, you can generate fillable forms directly in Google Drive. No need to leave Google Drive to make edits or sign documents, including blank ada dental claim form. Use pdfFiller's features in Google Drive to handle documents on any internet-connected device.
Can I sign the blank ada dental claim form 2017 electronically in Chrome?
You can. With pdfFiller, you get a strong e-signature solution built right into your Chrome browser. Using our addon, you may produce a legally enforceable eSignature by typing, sketching, or photographing it. Choose your preferred method and eSign in minutes.
Can I edit fillable ada dental claim form on an Android device?
You can make any changes to PDF files, such as dental claim form 2018, with the help of the pdfFiller mobile app for Android. Edit, sign, and send documents right from your mobile device. Install the app and streamline your document management wherever you are.
Fill out your empty denal claim form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Blank Ada Dental Claim Form 2017 is not the form you're looking for?Search for another form here.
Keywords relevant to ada dental forms
Related to 2017 ada dental claim form fill online rintable fillable






If you believe that this page should be taken down, please follow our DMCA take down process
here
.
